65 yo female referred by GP for lymphocytosis.
FBC: Hb 139g/L, WCC 12x10^9/L, platelets 369x10^9/L
Please comment on Morphology:
Discuss your approach to this patient
Here are the flow results – please interprete?
Do you wish for extra flow markers?
Discuss your diagnosis and broadly outline your management of this patient.
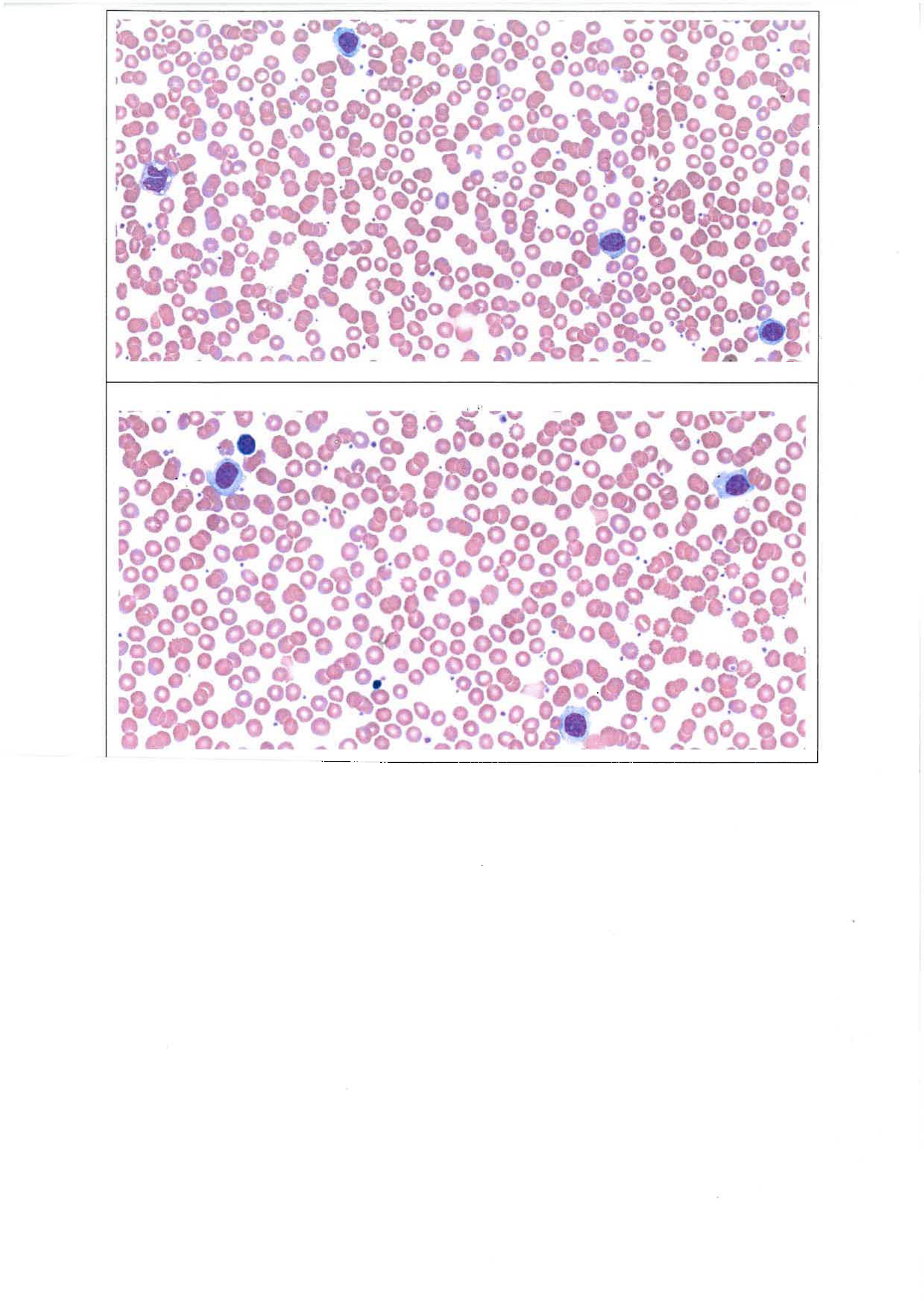
The haemoglobin and platelet count are well preserved with largely normal morphology. There is a mild lymphocytosis with medium sized cells with abundent basophilic cytoplasm some with cytoplasmic projections. there are some forms with prominent nucleoli.
Film features are suggestive of a lymphoproliferative disease such as Hairy cell Leukemia or variant given that some have prominent nucleoli. Other differential diagnoses include Splenic Marginal Zone Lymphoma, Chronic Lymphocytic Leukemia and Mantle cell Lymphoma.
Flow cytometry will be helpful to help clarify clonality of the lymphocytes and clarify diagnosis.
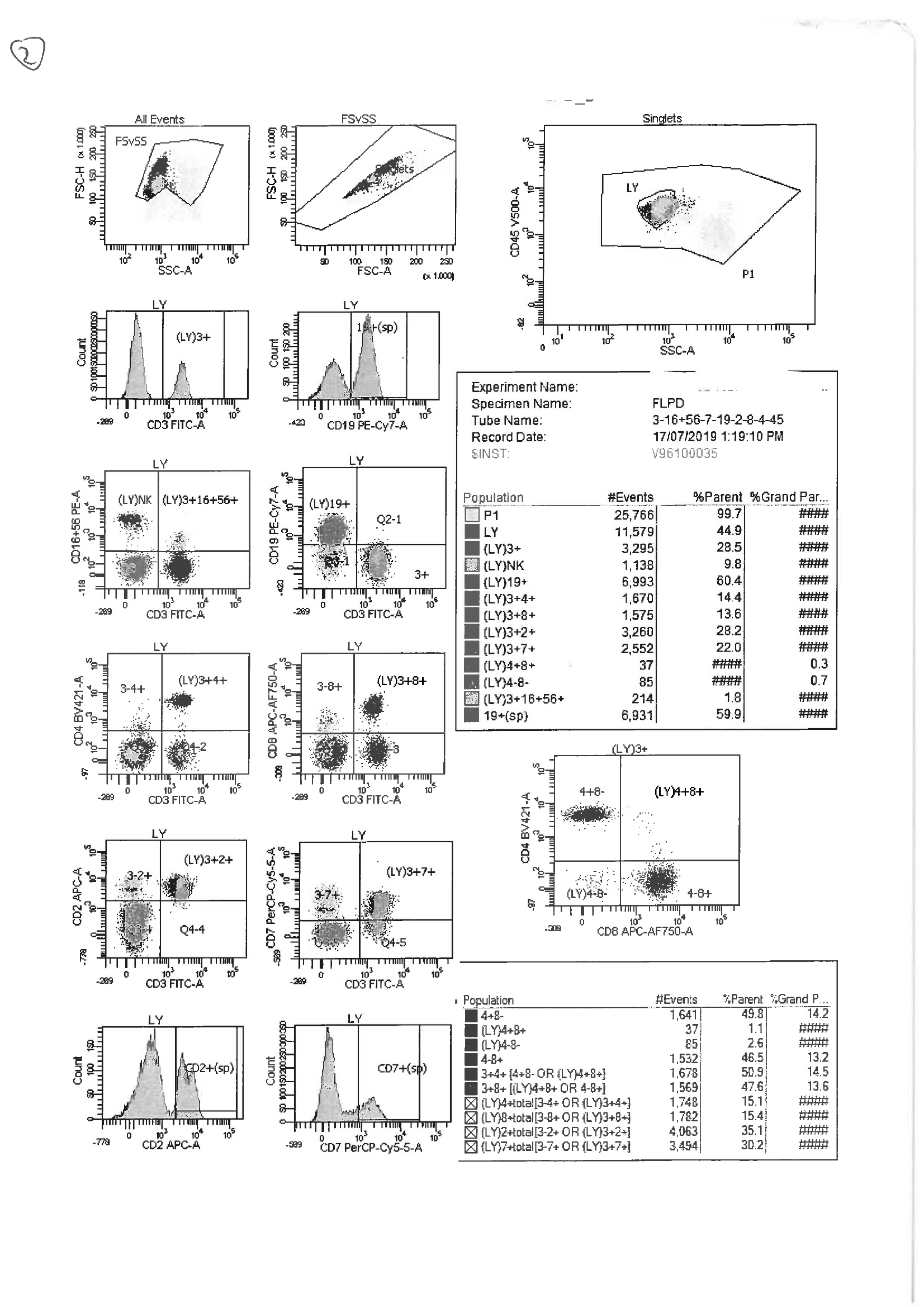
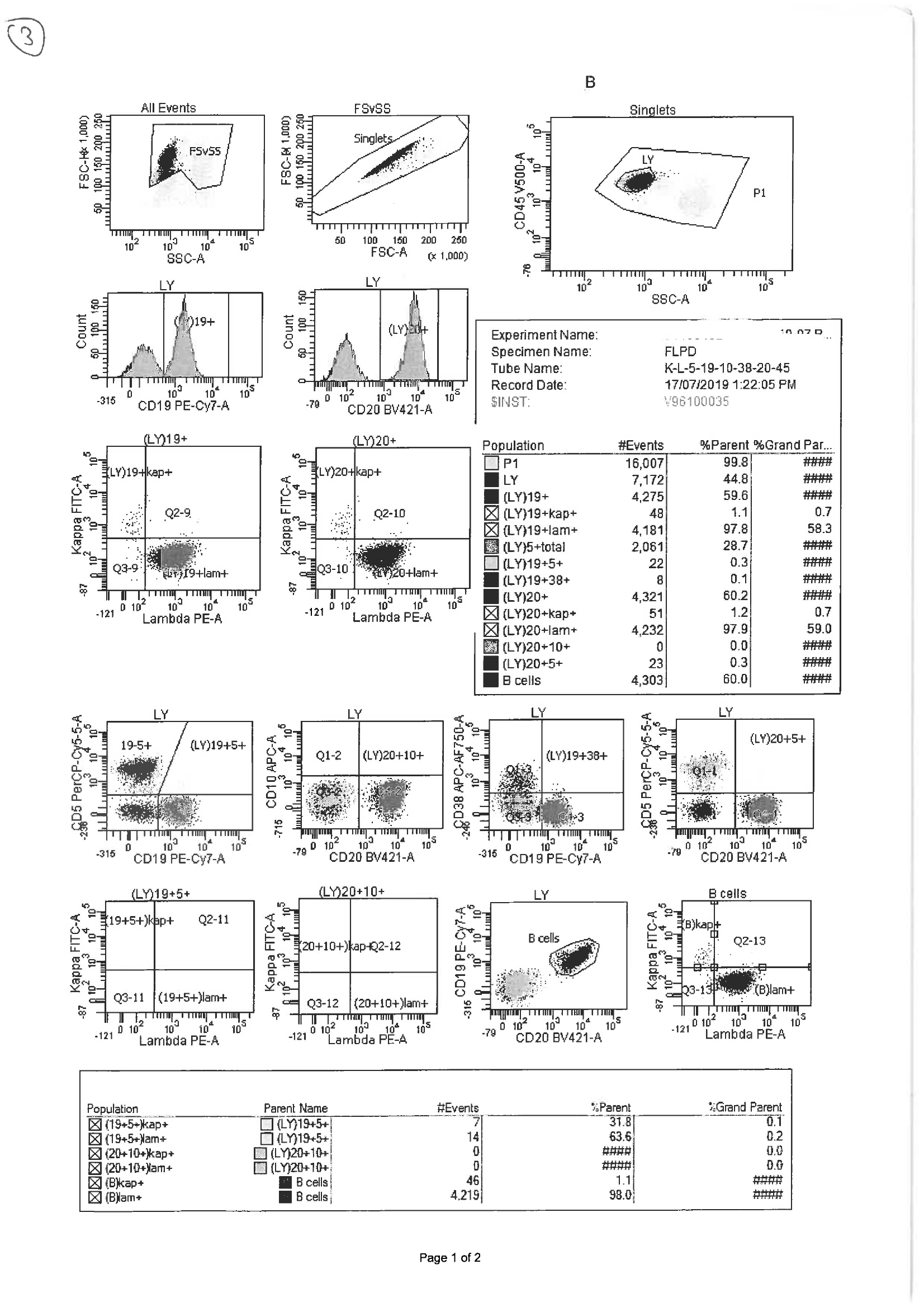
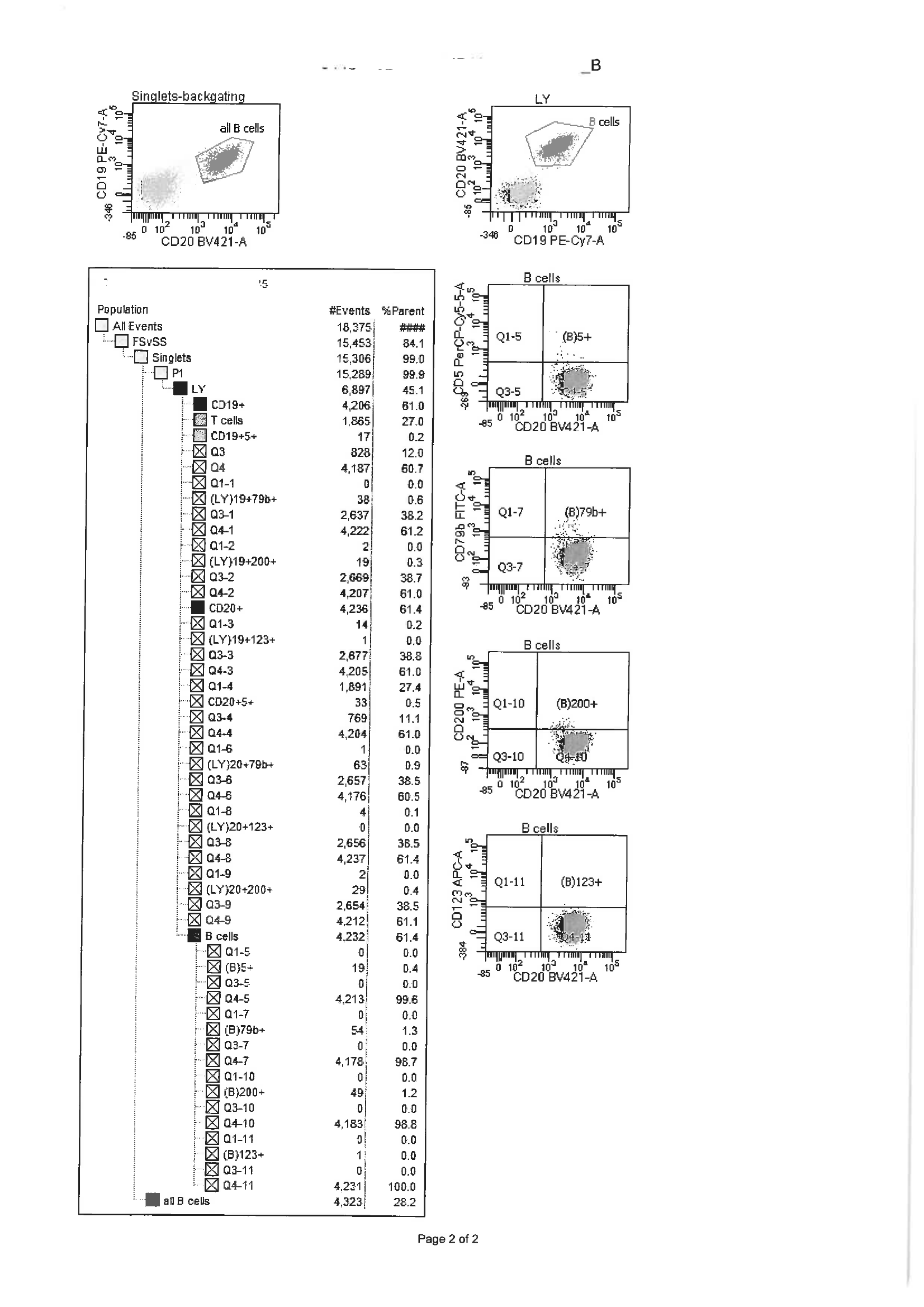
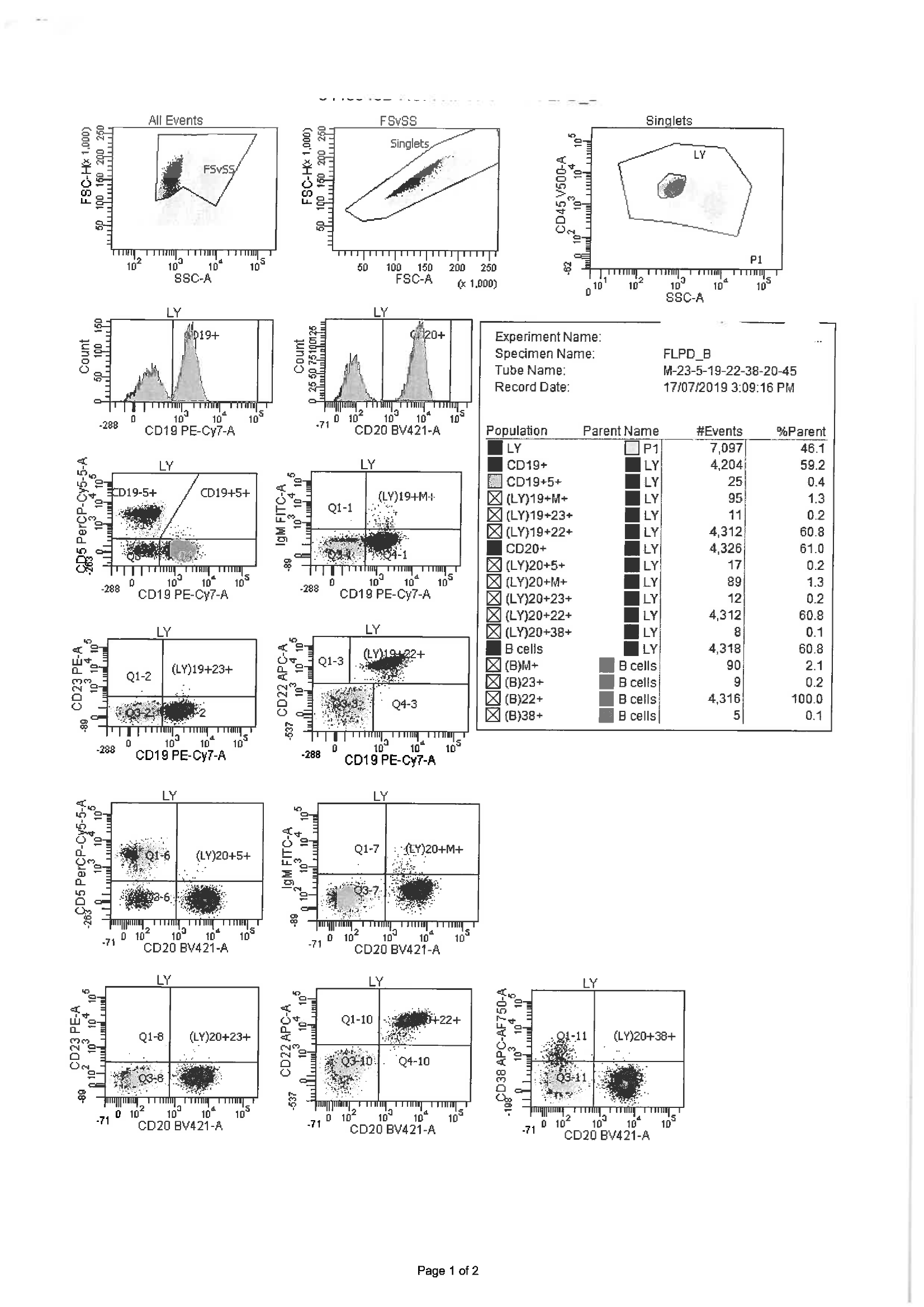
Flow cytometry shows 45% of cells gate as lymphocytes by CD45 and Side scatter analysis. 60% of the lymphocytes are clonal B cells expressing CD19, CD20 (bright) and CD22 positive and they are lambda light chain restricted. CD5, CD10, CD23, CD79b, CD200, CD123 and sIgM are negative as is CD38. 30% of the lymphocytes are T cells with normal surface antigenic expression.
These results are consistent with a B cell Lymphoproliferative Disorder. It rules out Chronic Lymphocytic Leukemia and Mantle Cell lymphoma and is suggestive of Hairy Cell Leukemia or variant given the bright CD20 positivity.
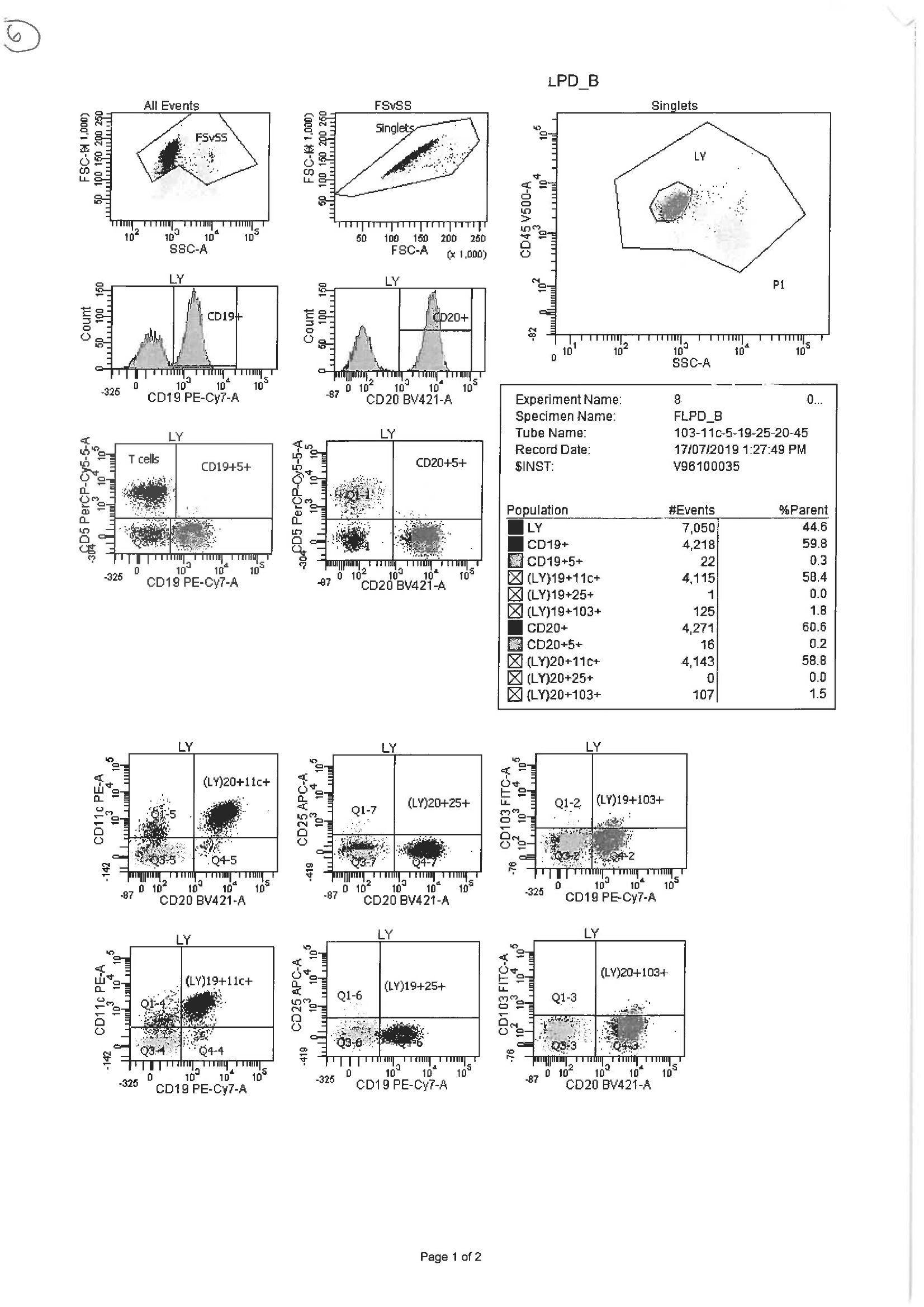
Hairy cell markers CD25, CD11c and CD103 should be ordered on the peripheral blood flow cytometry.
The clonal B cells are negative for CD25 and CD103 but are positive for CD11c. This is consistent with Hairy Cell Leukemia variant which is usually negative for CD25. The CD123 is also negative which is generally positive in HCL.
Bone marrow biopsy for BRAFV600E and Annexin A1 mutations should be negative.
Hairy Cell Leukemia variant is generally associated with a poorer prognosis and is less responsive to standard immunochemotherapy.
Management of this patient would include a watch and wait approach is he is stable or rituximab based or purine analogue based therapy is treatment is indicated.